
Full Text
Anomalous Left Coronary Artery from Right Sinus of Valsalva: An Anomaly with Fatal Outcomes
Muhammad Umer Awan1*, Muhammad Bilal Quraishi2, Nicky Wadiwala2, Niranjan Reddy31Resident Physician, Department of Internal Medicine Seton Hall University, St Francis Medical Center, Trenton, NJ, USA
2Cardiology Fellow, Department of Cardiovascular Medicine, Kettering Medical and Veterans Affairs Medical Center Dayton, Ohio, USA
3Associate Program Director Cardiology Fellowship, Kettering Medical and Veterans Affairs Medical Center Dayton, Ohio, USA
*Corresponding author: Muhammad Umer Awan, Resident Physician,Department of Internal Medicine Seton Hall University, St Francis Medical Center, Trenton,NJ, 08629, USA, Tel: 347-922-6970; E-mail: umer166@gmail.com
Article Information
Article Type: Case Report
Citation: Awan MU, Quraishi MB, Wadiwala N, Reddy N (2015) Anomalous Left Coronary Artery from Right Sinus of Valsalva: An Anomaly with Fatal Outcomes. J Heart Health, Volume1.1: http://dx.doi.org/10.16966/2379-769X.101
Copyright: © 2015 Awan MU, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Publication history:
Abstract
Coronary anomalies are not uncommon. Patients with coronary anomalies can have a wide array of presentations varying from chest pain to sudden cardiac death. In this case, a middle-aged woman presented with atypical chest pain and was admitted for unstable angina. Cardiac catheterization identified an anomalous origin of the left coronary artery from the right coronary sinus. CT angiogram identified a high-risk course. The patient’s chest pain was attributed to anomalous origin of the left coronary artery with subsequent compression due to inter-arterial course between the aorta and pulmonary trunk. She underwent successful surgical revascularization with left internal mammary artery to left anterior descending with resolution of symptoms.
Case Report
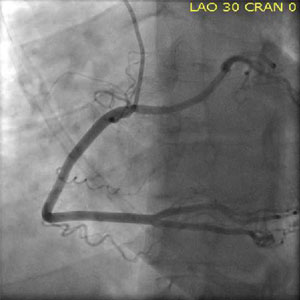
We report a case of a 48-year-old Caucasian female who presented to our facility for further evaluation of chest pain. The patient had developed severe substernal sharp pain radiating to her back. Her pain was self-reported to be eight on a scale from one to ten. Her family history was significant for myocardial infarction in all of her siblings in their 40’s and 50’s. A more detailed history revealed the patent had intermittent exertional chest pain for many years, which she had attributed to her asthma. On the day of presentation she experienced the worst pain of her life prompting her to seek medical attention. The patient was hemodynamically stable on presentation with negative cardiac markers and admitted with a diagnosis of unstable angina. Standard therapy resulted in marked improvement of her symptoms. On day two of admission, her troponins remained negative and electrocardiogram (EKG) showed no ischemic changes. She underwent cardiac catheterization via radial approach. Multiple attempts to engage the left system were unsuccessful followed by success full engagement of the right coronary artery (RCA) with the 5 French (5Fr) Jacky catheter (Figures 1 and 2). The right system showed no obstruction. Initially, an anomalous circumflex was thought to arise from the RCA; however an aortogram and ventriculogram failed to reveal the origin of the left system (Figure 3). Careful review of the angiograms suggested an absent left system and an anomalous origin of the left coronary artery from the opposite ostia (ACAOS). Otherwise the coronaries had no angiographically definable stenosis. A CT coronary angiogram was done to delineate the course. This confirmed absence of the left coronary artery and anomalous origin of left coronary artery from opposite ostia (Figures 4a and 4b). The artery had an inter-arterial anteroposterior course between the aorta and pulmonary trunk suggesting compression of the left main artery as a possible mechanism of the patient’s intermittent exertional chest pain. The patient underwent successful surgical revascularization with LIMA to LAD after which she experienced no more pain.
Discussion
Coronary anomalies remain the second most common cause of sudden cardiac death (SCD) after hypertrophic cardiomyopathy in children and young athletes with most diagnoses made at autopsy [1]. In adults, coronary anomalies are most commonly identified as incidental findings at cardiac catheterization. Although the incidence of coronary anomalies is approximately 5.64%,
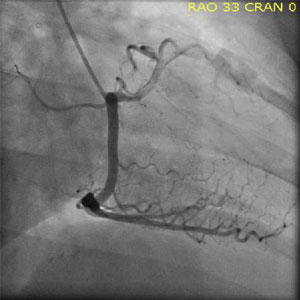
Figure 2. RAO Cranial view of RCA and anomalous origin of left coronary artery from opposite sinus
not all are associated with poor outcomes [2]. ACAOS remains the most feared with 0.92% comprising of anomalous origin of RCA from the left sinus and 0.15% incidence of anomalous origin of left coronary artery from the right sinus [2].
Young athletes with ACAOS experience SCD from vigorous exercise which sets up a plethora of hemodynamic changes. These changes compromise the anatomical integrity of ACAOS especially if the course is inter-arterial. In one of the largest series ever reported of eighteen year old military recruits undergoing intense military training for eight weeks, 277 non trauma related deaths were identified. Of these, 64 were cardiac deaths, 21 of which were related to left ACAOS. No other coronary anomaly was associated with death. This and many other series suggest SCD as the primary presentation in young athletes [3-6]. Adults may remain asymptomatic or have chest pain with typical or atypical symptoms [7].
Numerous mechanisms have been proposed. Angelini contests the popular notion of compression being the sole reason for intermittent ischemia. He proposes intussusceptions as the underlying mechanism as the anomalous artery lies inside the arterial wall i.e. intramural. He cites coronary hypoplasia of the proximal intramural portion of ACAOS to be prone to intussusception. The intramural segment is also ovoid rather than circular, which has a smaller cross sectional area, hence lateral compression generated from hemodynamic stresses may occur. Lastly, segmental stenosis varying from 5-15 mm may exist. These salient features have been shown to be associated with intussusception of left ASAOS verified by intravascular ultrasound assessment [1].
The management of symptomatic left ACAOS remains surgical [8]. However, a few cases of stenting have been reported [9,10]. When stenting is the method of revascularization, deployment should be under IVUS guidance. Post-deployment IVUS should be done to ensure the stent struts are well apposed. Our patient underwent surgical revascularization with LIMA to LAD. She had an uncomplicated course and reported no further chest pain at 30-day follow-up.
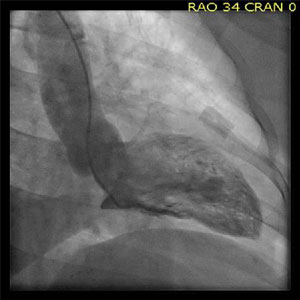
Figure 3. Aortogram and ventriculogram revealing Origin of RCA and anomalous origin of left coronary artery from opposite sinus

Figure 4a. CT coronary angiogram showing Inter arterial course of left ACAOS

Figure 4b. CT coronary angiogram showing Inter arterial course of left ACAOS
References
- Liesting C, Brugts JJ, Kofflard MJ, Dirkali A (2012) Acute coronary syndrome in a patient with a single coronary artery arising from the right sinus of valsalva. World J Cardiol 4: 264-266.[Ref.]
- Angelini P (2007) Coronary artery anomalies: An entity in search of an identity. Circulation, 115: 1296-1305.[Ref.]
- Meel BL (2011) An anomalous origin of left coronary artery and sudden death in a soccer player: A case report. Med Sci Law, 51: 182-183.[Ref.]
- Nguyen AL, Haas F, Evens J, Breur JM (2012) Sudden cardiac death after repair of anomalous origin of left coronary artery from right sinus of valsalva with an interarterial course: Case report and review of the literature. Neth Heart J, 20: 463-471.[Ref.]
- Pavlidis AN, Karavolias GK, Malakos JS, Sbarouni E, Georgiadou P, et al. (2012) Anomalous origin of coronary arteries: When one sinus fits all. Acute Card Care. 14: 99-102.[Ref.]
- Penalver JM, Mosca RS, Weitz D, Phoon CK (2012) Anomalous aortic origin of coronary arteries from the opposite sinus: A critical appraisal of risk. BMC Cardiovasc Disord 12: 83.[Ref.]
- Eckart RE, Scoville SL, Campbell CL, Shry EA, Stajduhar KC, et al. (2004) Sudden death in young adults: A 25-year review of autopsies in military recruits. Ann Intern Med, 141: 829-834.[Ref.]
- Colak MC, Erdil N, Disli O, Kahraman E, Battaloglu B (2012) Anomalous origin of the left coronary artery from the right coronary sinus. Ann Thorac Cardiovasc Surg, 18: 548-550.[Ref.]
- Charan L, Shiradkar S, Kerkar PG, Ashish A (2011) Stenting of anomalous left main coronary artery stenosis in an adult with a retroaortic course. Cardiol Res Pract, 296946.[Ref.]
- Chen M, Hong T, Huo Y (2005) Stenting for left main stenosis in a child with anomalous origin of left coronary artery: Case report. Chin Med J (Engl), 118: 80-82.[Ref.]
Download Provisional pdf here
SCI FORSCHEN JOURNALS
All Sci Forschen Journals are Open Access
New Journals
Best viewed in Google Chrome | Mozilla Firefox | Microsoft Edge
Copyright © 2024 Sci Forschen Inc., All Rights Reserved